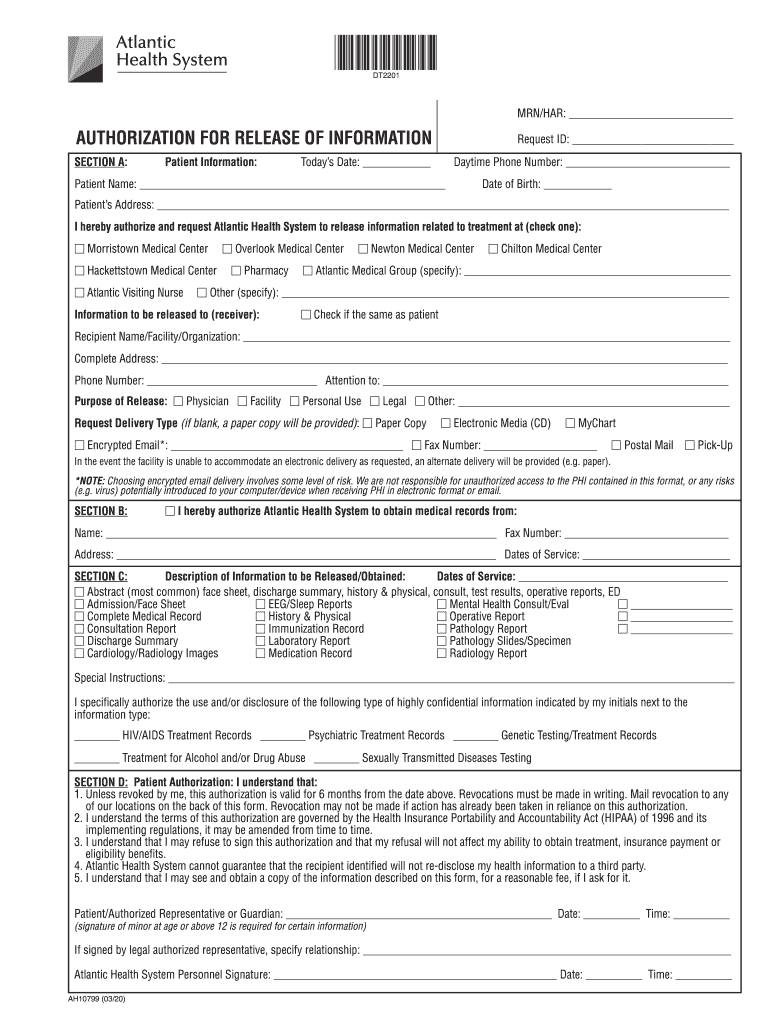
disclosure authorization form
transfer agreement for trauma services
Aug 31, 2021 (a). Name, address and age of patient;. (b). Name address and telephone number of patients next of kin;. (c). Available history;. (d). RecordsRead more
Learn more
Health Safety Requirements
Mar 9, 2026 If a representative is chosen, an authorization form will need to be submitted during the appointment. Parents also have the option of callingRead more
Learn more
Request for Proposal No. RS-IRM-97-195 Entitled
Dec 11, 1997 (3) Review all costs requested for reimbursement by the contractor and submit to the contracting officer recommendations for approval,Read more
Learn more