


Definition and Purpose of the Medi-Cal Choice Form
The Medi-Cal Choice Form is used to join or change health plans under the California Department of Health Care Services. It is an essential document for residents of California who are eligible for Medi-Cal, allowing them to select or switch their healthcare plans. The form gathers critical personal information from applicants, which includes contact details, current and preferred managed care plans, as well as reasons for any requested changes in plans. Understanding its structure and components is crucial for applicants to ensure accurate submission.
How to Use the Medi-Cal Choice Form
To effectively use the Medi-Cal Choice Form, applicants must begin by gathering all necessary personal information likely needed on the form. This includes details such as full name, date of birth, and existing health plan specifics. Filling out the form requires attention to sections that ask for health plan preferences and the rationale for changes, if applicable. Once completed, it is important to review each section for accuracy before submission to avoid processing delays.
Obtaining the Medi-Cal Choice Form
The Medi-Cal Choice Form is accessible through multiple channels. Applicants can obtain a copy by visiting the official website of the California Department of Health Care Services. Alternatively, physical forms can be acquired from local county social services offices. It may also be possible to request forms by calling the health plan's member services or through other designated community resources that assist with Medi-Cal applications.
Step-by-Step Instructions to Complete the Medi-Cal Choice Form
-
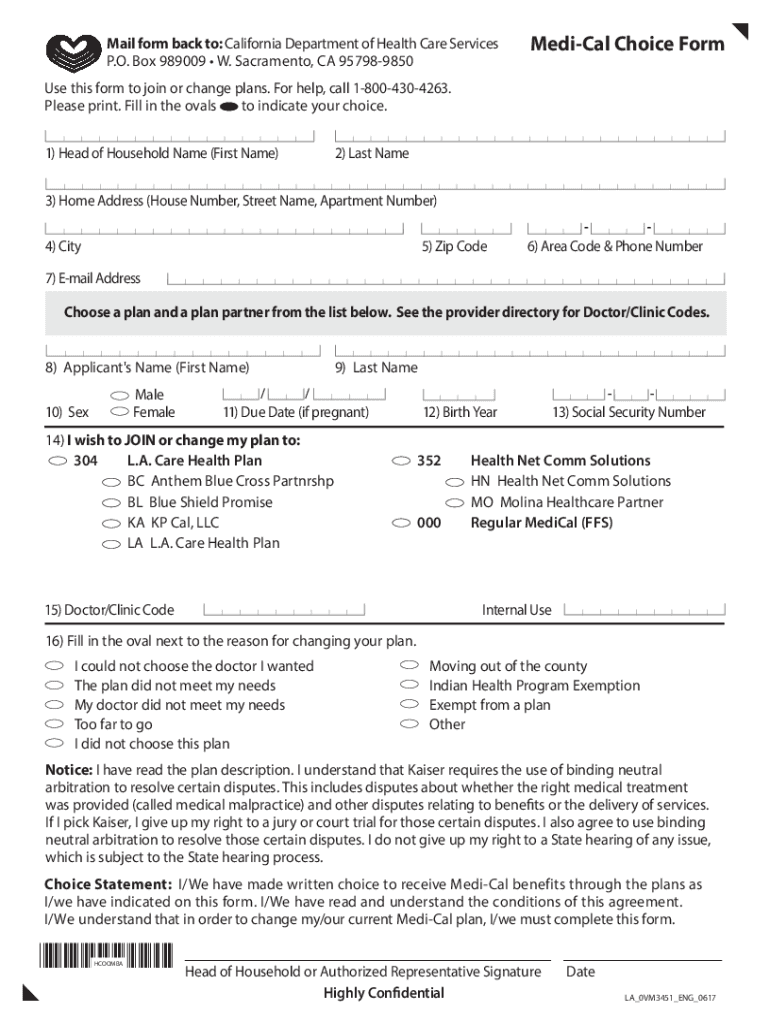
Personal Details: Begin by entering your full name, date of birth, and Medi-Cal identification number.
-
Current Health Plan Information: Provide information about your current health plan and reason for choosing to change if applicable.
-
Selection of New Health Plan: Choose your preferred health plan from the options available in your county. Where applicable, rank your choices if there are multiple preferences.
-
Reason for Change: Specify reasons for changing plans, such as seeking better service or needing to stay with current healthcare providers.
-
Signature: Sign and date the form to confirm the information provided is accurate and truthful.
-
Submission: Submit the form via mail, in-person drop-off at a designated office, or through an approved online platform.
Importance of Filling Out the Medi-Cal Choice Form
Filling out the Medi-Cal Choice Form correctly is important as it directly affects access to healthcare benefits. Making informed choices regarding health plans can lead to better healthcare outcomes and satisfaction with the level of care received. Additionally, completing the form thoroughly ensures compliance with state requirements, preventing any interruptions in health coverage.
Typical Users of the Medi-Cal Choice Form
The form is primarily used by individuals eligible for Medi-Cal in California, including those who are newly qualifying or existing beneficiaries looking to change their health plans. It is particularly relevant for low-income families, elderly citizens, persons with disabilities, and qualified immigrants who receive state-managed health insurance.
Key Elements of the Medi-Cal Choice Form
- Personal Information Section: Details about the applicant, such as name, contact information, and Medi-Cal ID.
- Health Plan Selection: Options to select a new or change an existing health plan.
- Reason for Selection/Change: Space to provide reasons for health plan choices or changes.
- Signature Area: Mandatory confirmation through signature to finalize the form.
- Privacy Notice: Explanation of how personal information will be used and protected under California law.
State-Specific Rules for the Medi-Cal Choice Form
California has specific guidelines regarding eligibility and submission of the Medi-Cal Choice Form. Applicants must meet state residency requirements and fall under specific income categories to qualify for Medi-Cal. Furthermore, the state dictates the managed care health plans available to applicants based on county of residence, influencing the choices listed on the form.
Examples and Scenarios for Using the Medi-Cal Choice Form
Consider a scenario where an elderly applicant is already under a Medi-Cal health plan but wishes to transition to a different plan due to moving to a new county. The form would allow this individual to select a new plan that better accommodates their new geographic location. Another case could involve a low-income family seeking a health plan that includes specialized pediatric services, necessitating a switch using the form.