


Definition and Importance of the Nursing Visit Record
A nursing visit record is a critical document that captures essential data regarding a patient's health status during home healthcare visits. This form serves as a primary tool for nurses to document observations, assessments, and care provided to the patient. It functions not just as a record for the care delivered, but also aids in continuity of care among healthcare providers.
Key Features of a Nursing Visit Record
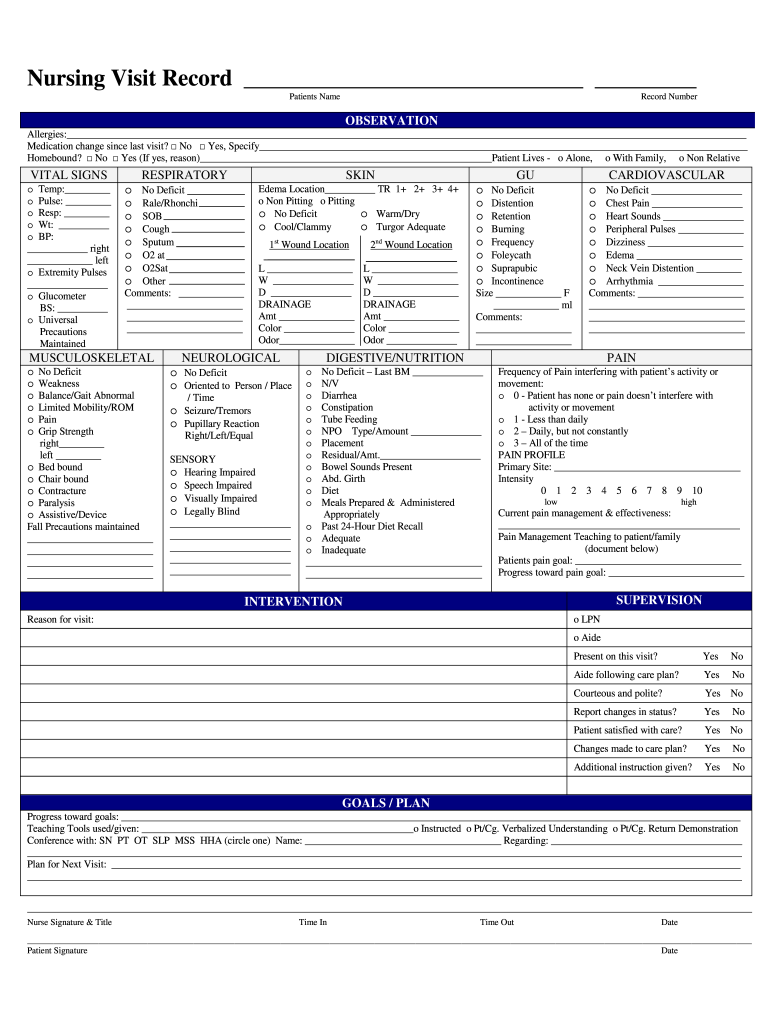
- Patient Identification: Each record includes demographic information about the patient, such as name, age, and medical history. This helps healthcare professionals quickly ascertain the patient's background.
- Vital Signs and Observations: Nurses record vital signs like temperature, pulse, and blood pressure, providing a snapshot of the patient's health at the time of visit.
- Assessment of Health Systems: The form allows nurses to evaluate various health systems, including respiratory, cardiovascular, and neurological assessments. This thoroughness is crucial for identifying acute or chronic medical issues.
- Pain Management Documentation: A section is dedicated to pain management strategies, enabling nurses to report the patient's pain levels and interventions that have been implemented.
- Intervention Notes: Nurses can write down specific interventions performed during the visit, such as medication administration or wound care, ensuring all actions taken are documented.
Importance of Comprehensive Documentation
Having accurate records:
- Aids not just in patient care but also in legal compliance.
- Provides valuable insights for future healthcare decisions and treatment plans.
- Supports coordination among healthcare providers, enhancing collaborative care.
How to Effectively Use the Nursing Visit Record
Utilizing the nursing visit record effectively enhances care quality and ensures comprehensive documentation of patient interactions.
Steps to Use the Nursing Visit Record
- Pre-visit Preparation:
- Gather relevant patient information and previous records.
- Ensure the nursing visit record form is readily accessible, whether in digital or paper form.
- During the Visit:
- Systematically fill out the form as observations are made. This includes noting vital signs, assessments, and any procedures carried out.
- Engage with the patient or caregiver to obtain accurate details and context regarding the patient's condition and care needs.
- Post-visit Completion:
- Review the completed nursing visit record to confirm all sections are filled out accurately.
- Ensure that notes are legible and free from ambiguity, which could aid in future visits.
Best Practices for Using Nursing Visit Records
- Consistency: Use the record consistently for each patient visit to establish a comprehensive care timeline.
- Confidentiality: Protect the patient’s information in compliance with HIPAA regulations to maintain confidentiality.
Legal Use of the Nursing Visit Record
Nursing visit records hold significant legal implications in healthcare. They serve as legal documents that can be referenced in case of disputes, audits, or quality assessments.
Legal Considerations
- Compliance with Standards: Nursing documentation must adhere to state and federal regulations. This ensures that all entries are legally acceptable for review by regulatory bodies.
- Evidence in Legal Proceedings: A well-maintained nursing visit record can support a nurse's actions in legal situations. Accurate documentation can demonstrate adherence to standards of care and clinical protocols.
- Retention Policies: Many states have specified guidelines for how long healthcare records, including nursing visit records, must be retained.
Importance in Quality Assurance
- Nurses use the records to review care quality and ensure adherence to best practices. Auditors and inspectors may reference these records to assess compliance with healthcare standards.
Key Elements of the Nursing Visit Record
Understanding the critical components of the nursing visit record is essential for complete and effective documentation.
Major Components Included in the Nursing Visit Record
- Identification Information: Name, date of birth, and insurance details.
- Date and Time of Visit: Important for tracking follow-up schedules and documentation timelines.
- Assessment Data: Documented vital signs, patient complaints, and health system assessments.
- Intervention Records: Outline the specific care delivered during the visit, including medications administered or changes in treatment.
- Follow-up Plans: This section outlines future interventions, care goals, and any referrals made to other healthcare professionals.
Relevance of Each Element
Each component ensures comprehensive care documentation, promoting continuity and quality of care over time. This format allows for easy comparisons in patient health status during subsequent visits.
Examples of Using the Nursing Visit Record
Practical examples can illuminate how nursing visit records streamline healthcare delivery and improve patient outcomes.
Case Studies on Nursing Visit Records
- Case of Chronic Condition Management: A nurse visits a patient with congestive heart failure. The nursing visit record captures relevant vital signs, including weight changes and edema levels, which inform medication adjustments and follow-up strategies.
- Post-surgical Care Record: In the case of a post-operative patient, the nursing visit record documents pain levels, incision inspection, and patient education regarding wound care, ensuring a clear communication of care protocols.
Benefits of Documented Examples
- By analyzing previous records, healthcare providers can identify patterns in patient health, which can lead to improved care strategies.
- The record also serves as a historical account, guiding future treatment decisions and care plans.
State-specific Rules for the Nursing Visit Record
Nursing visit record requirements can vary significantly from state to state, emphasizing the need for medical professionals to be well-informed about their local regulations.
Understanding State Regulations
- Record Keeping: Different states may have unique guidelines regarding certain elements that must be recorded in the nursing visit record.
- Confidentiality Laws: Providers must be aware of specific regulations centered around patient data privacy that pertain to their state.
Implications for Nurses
- Being informed about local laws ensures that nurses not only comply with legal standards but also deliver quality patient care within those frameworks.
- Non-compliance can result in legal repercussions or penalties, making it crucial for nursing professionals to stay educated about evolving regulations.
This exploration of the nursing visit record reflects its multi-faceted role in healthcare documentation, emphasizing its importance for care quality, legal compliance, and patient outcomes across the home healthcare setting.