


Definition and Meaning of the Nursing Report Sheet Template
The nursing report sheet template is a structured document used by healthcare professionals, primarily nurses, to consolidate and communicate crucial patient information during shift changes. This standardized format ensures that every nurse has access to relevant details, which enhances patient care and safety. The report sheet often includes sections for patient demographics, vital signs, medications, care plans, and any specific notes or observations.
Understanding this template's purpose allows nurses to quickly assess patient status and prioritize care needs effectively. The use of a nursing report sheet template facilitates a streamlined communication process, minimizing the chance of errors during patient handoffs. By utilizing a consistent format, nursing staff foster a culture of accountability, ensuring that critical information is always communicated.
Key Elements of the Nursing Report Sheet Template
A well-designed nursing report sheet template includes several key elements that provide a comprehensive view of patient care. The most common components are:
- Patient Demographics: Basic patient information such as name, age, gender, and identification details.
- Medical History: A summary of relevant past medical history, allergies, and comorbidities that impact current care.
- Vital Signs: Recent measurements of blood pressure, heart rate, temperature, and respiratory rate, vital for assessing patient stability.
- Medications: A list of current medications, dosages, and the schedule for administration to prevent errors.
- Care Plans: Individualized care goals and interventions, allowing nurses to understand the intended care trajectory for each patient.
In many templates, additional sections may be included for abnormal findings, planned procedures, and nursing assessments, ensuring that nurses have all necessary information readily accessible, supporting accurate patient evaluations.
How to Use the Nursing Report Sheet Template
Using the nursing report sheet template involves several steps to ensure effective documentation and communication. Here’s how to utilize the template efficiently:
- Collect Information: Before the shift begins, gather all necessary documents, including previous report sheets, patient records, and any outstanding orders.
- Fill in Patient Details: Input essential patient demographics, ensuring the information is accurate and complete.
- Document Vital Signs: Record up-to-date vital signs as this data is crucial for evaluating patient health status during handoffs.
- List Medications: Ensure all medications are logged correctly, highlighting any changes in dosage or new prescriptions.
- Update Care Plans: Review the existing care plans and update any outcomes or ongoing strategies to provide context for incoming staff.
Following this structured approach helps maintain a clear line of communication among nursing staff, which is essential for delivering quality patient care.
Important Terms Related to the Nursing Report Sheet Template
Familiarity with specific terminology associated with the nursing report sheet template enhances comprehension and facilitates effective communication among healthcare providers. Key terms include:
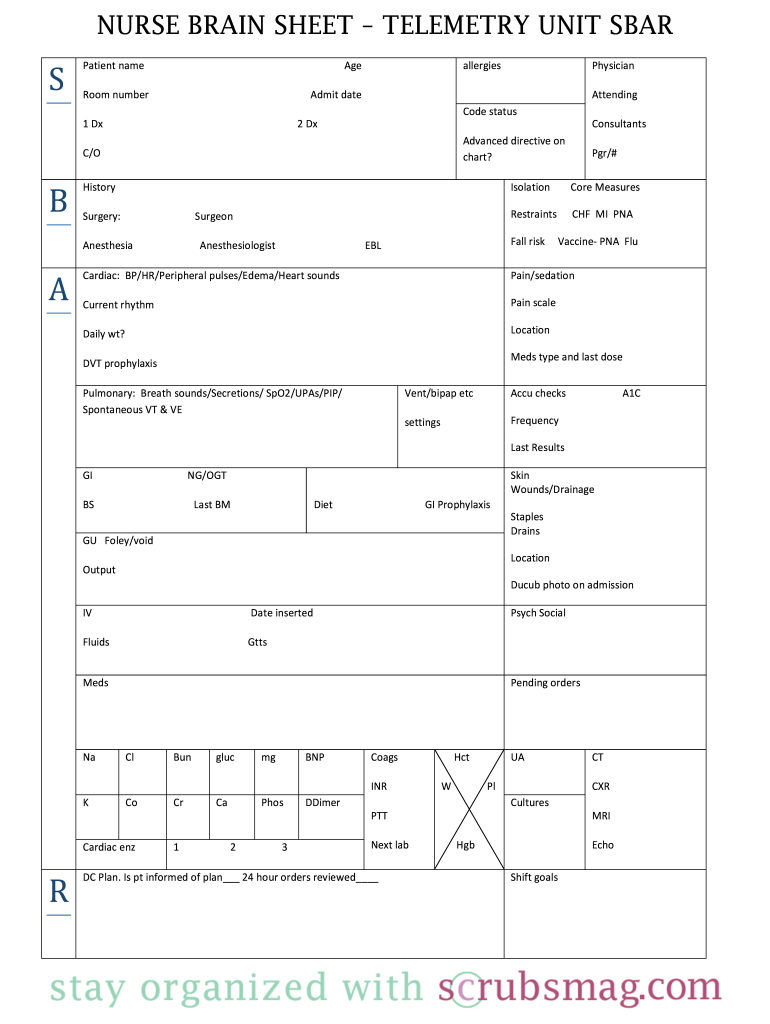
- SBAR: A communication framework (Situation, Background, Assessment, Recommendation) commonly employed in nursing to provide structured and concise patient information.
- Vital Signs: Measurements of bodily functions indicating the state of a patient's essential physiological parameters, including heart rate and blood pressure.
- Charting: The process of documenting patient data in a medical record, which is critical for legal and clinical purposes.
- Care Plan: A written approach tailored to meet a patient's healthcare needs, outlining specific interventions and goals.
Understanding these terms is vital for nurses to communicate effectively, maintain patient safety, and ensure continuity of care.
Examples of Using the Nursing Report Sheet Template
Practical examples of using a nursing report sheet template can illustrate its versatility in real-world scenarios. Here are a few situations where this tool proves especially useful:
- Shift Handoffs: During a busy shift change, a nurse may use the report sheet template to summarize critical patient information quickly, ensuring that incoming staff members are aware of any immediate concerns.
- ICU Settings: In intensive care units, a more detailed report sheet may be utilized to document intricate patient information, including titration of drips and the frequency of monitoring essential due to the high-acuity nature of patients.
- Multidisciplinary Rounds: Nurses can enhance communication during rounds by presenting summaries from their report sheets, allowing all team members to understand patient goals and progress.
- Emergency Situations: In an urgent care setting, having a comprehensive report sheet readily available can expedite decision-making, aiding rapid assessment and intervention.
These examples highlight the flexibility and importance of using a nursing report sheet template across diverse nursing contexts.
Steps to Complete the Nursing Report Sheet Template
Completing the nursing report sheet template involves a clear and methodical process to ensure its effectiveness in communication. Below are the steps typically followed:
- Pre-Shift Preparation: Before the shift starts, review previous reports and patient charts to gather necessary baseline information.
- Customize the Template: Adjust the report sheet template as needed to fit specific unit requirements or patient loads.
- Incorporate Accurate Data: Fill in patient names, dates, and vital signs systematically, taking care to avoid omissions or errors that could impact patient care.
- Highlight Critical Information: Use bold text or utilize color coding to make essential information noticeable, such as allergies or code status.
- Secure Signatures: In team settings, ensure that all nurses involved sign the report sheet, indicating their acknowledgment of the patient's status.
Following these steps helps in constructing a thorough and effective nursing report sheet, ensuring seamless communication amongst the nursing team.

