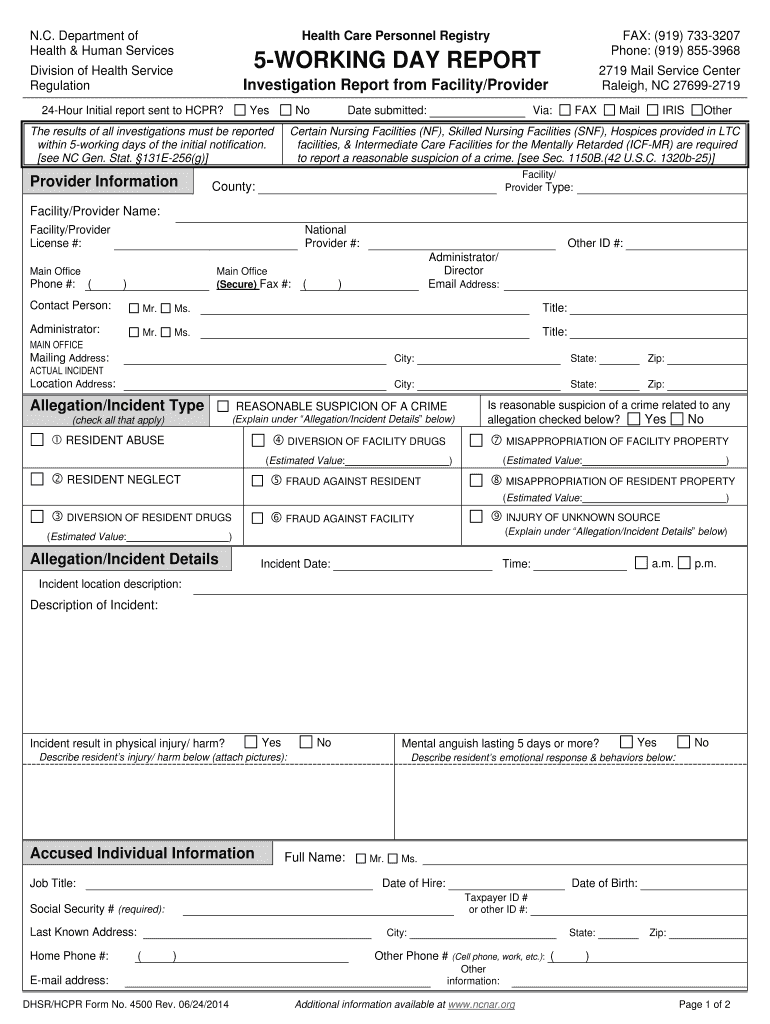
printable 24 hour report sheet nursing home
NURSING FACILITY REPORTED INCIDENTS (FRI)
What is to be reported: 1. All alleged violations involving abuse, neglect, exploitation or mistreatment, including injuries of unknown source andRead more
Learn more
Toolkit on State Actions to Mitigate COVID-19 Prevalence in
Feb 1, 2021 This toolkit catalogs the many innovative solutions designed at the state level to protect our nations vulnerable nursing home residents duringRead more
Learn more
Templates | Graphic Standards | UC Davis Health
Use these sample templates and examples to help guide you in making consistent UC Davis Health branded marketing collateral.Read more
Learn more