


Definition and Meaning of the Brain Nursing Report Sheet
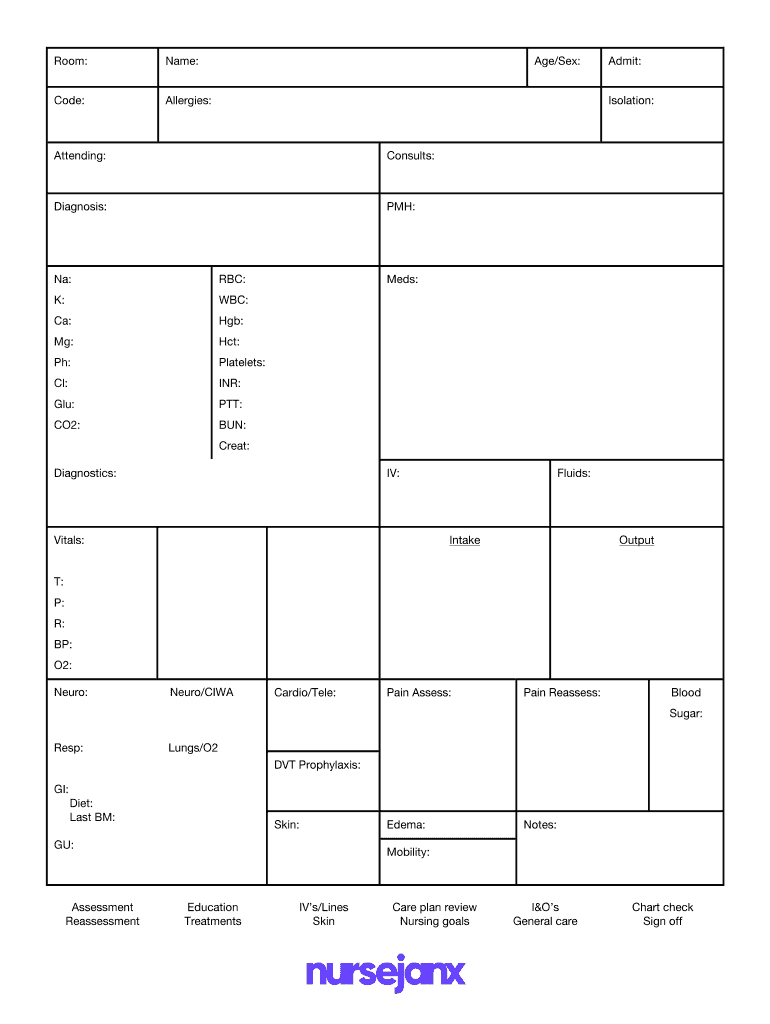
The Brain Nursing Report Sheet is a structured document used primarily in healthcare settings to facilitate the organization and communication of patient care information among nursing staff. This document serves as a crucial tool for nurses to track critical patient data during their shifts, ensuring that all aspects of patient care are addressed and monitored effectively. The sheet typically includes sections for vital signs, medication administration, patient history, assessments, and real-time updates on patient status.
For healthcare providers, the Brain Nursing Report Sheet is not merely a recording tool but an integral component of the nursing process that promotes continuity of care. By standardizing the way information is recorded, it helps nurses and nursing aides quickly reference important patient details, reducing errors and enhancing patient safety.
How to Use the Brain Nursing Report Sheet
Using the Brain Nursing Report Sheet involves several important steps. Nurses typically begin by entering each patient's basic information, such as name, age, identification number, and diagnosis. This initial setup is foundational for the effective use of the sheet throughout their shift.
Once the basic information is in place, nurses fill out key sections:
- Vital Signs: A continuous recording of the patient's vital signs, such as blood pressure, heart rate, temperature, and respiratory rate, allows nurses to quickly assess patient condition changes.
- Medications: Keeping track of medications administered, along with their dosage and administration time, ensures compliance with treatment plans.
- Assessments: Nurses conduct regular assessments, documenting findings directly on the sheet to maintain a real-time log of care and observations.
To enhance function, nurses often implement a color-coding system to symbolize patient statuses—green for stable, yellow for caution, and red for critical—making it easy to identify the need for urgent attention.
Who Typically Uses the Brain Nursing Report Sheet
The Brain Nursing Report Sheet is predominantly utilized by registered nurses (RNs) and licensed practical nurses (LPNs) in various healthcare settings, including:
- Hospitals: Inpatient nursing units where continuous and comprehensive patient care is pivotal.
- Long-Term Care Facilities: Such as nursing homes, where chronic patient management and daily care planning are essential.
- Home Health Agencies: Enabling nurses to efficiently monitor multiple patients over varied locations.
- Emergency Departments: Providing a quick overview of patient statuses for triaging and immediate treatment decisions.
Additionally, nursing students and educators may use the sheet as a teaching tool to familiarize learners with patient data management and interdisciplinary communication.

Key Elements of the Brain Nursing Report Sheet
Understanding the essential components of the Brain Nursing Report Sheet enhances its utility. Common elements include:
- Patient Identification: Includes necessary demographic details for easy identification.
- Assessment Section: Captures critical observations regarding the patient's condition and response to treatment.
- Plan of Care: Outlines the intended interventions, including medications, treatments, and follow-up assessments.
- Communication Log: Provides space for notes, ensuring seamless communication between shifts and team members.
These key elements contribute to a holistic view of patient care, allowing nurses to make informed decisions based on comprehensive data.
Steps to Complete the Brain Nursing Report Sheet
Completing the Brain Nursing Report Sheet effectively requires attention to detail and a systematic approach. Here are the steps to ensure accurate documentation:
-
Initial Setup: Collect and enter necessary patient details at the beginning of each shift. This includes demographic information and any new admissions or transfers.
-
Regular Updates: Continuously record vital signs as they are obtained throughout the shift. Adhere to scheduled times for medication administration, noting any changes in the patient's condition.
-
Conduct Assessments: Once an hour or per hospital policy, assess patients and document findings immediately. Make note of any significant changes that may require rapid intervention.
-
Interdisciplinary Notes: Record any relevant communications from physicians, specialists, or other healthcare professionals to maintain an accurate picture of the patient’s care plan.
-
Shift Handover: At the end of the shift, summarize the report for incoming staff. This handover is crucial for ensuring that all patient needs are met and that ongoing treatment plans are adhered to.
By following these steps diligently, nurses enhance patient safety and ensure effective collaboration across the healthcare team.
Important Terms Related to the Brain Nursing Report Sheet
Familiarity with specific terminology associated with the Brain Nursing Report Sheet aids in better comprehension and efficient usage. Important terms include:
- Charting: The process of documenting patient care and observations.
- SBAR: An acronym for Situation, Background, Assessment, Recommendation, which structures communication between healthcare professionals.
- Care Plan: A strategy outlining how healthcare providers will address the needs of a patient during their care.
- Interventions: Actions taken based on assessments to improve patient outcomes.
- EHR Integration: The incorporation of information from electronic health records to provide a cohesive view of patient care.
Understanding these terms supports nurses in utilizing the report sheet effectively and enhances the quality of communication within the healthcare team.
Examples of Using the Brain Nursing Report Sheet
Practical application of the Brain Nursing Report Sheet can be seen in various scenarios. Here are several examples:
-
Scenario 1: A nurse on a medical surgical unit uses the sheet to track a post-operative patient who requires complex care. Each vital sign measurement is logged, and medication doses are meticulously documented along with responses to pain management.
-
Scenario 2: In a long-term care facility, the nursing staff utilizes the sheet to manage multiple patients’ daily care needs. By recording each resident's status in real-time, they can prioritize care and address urgent matters efficiently.
-
Scenario 3: During shift change in an emergency department, a nurse uses the Brain Nursing Report Sheet to provide a comprehensive overview to incoming staff about patients under critical observation. Key interventions and vital signs are reviewed, allowing for smooth continuity of patient care.
These scenarios illustrate the versatility and essential role of the Brain Nursing Report Sheet in various healthcare environments.
Legal Use of the Brain Nursing Report Sheet
The legal use of the Brain Nursing Report Sheet is paramount to protect patient confidentiality and ensure compliance with regulatory standards.
-
HIPAA Compliance: The Health Insurance Portability and Accountability Act mandates strict guidelines for the protection of patient information. Hence, any notes or documentation must be handled and stored securely to avoid unauthorized access.
-
Documentation Standards: Accurate and timely documentation protects healthcare professionals in the event of legal scrutiny. Failure to provide complete records may result in liability if disputes arise regarding patient care.
-
Retention Policies: Healthcare facilities generally maintain their own policies regarding how long documentation should be retained. Nurses should familiarize themselves with these policies to ensure compliance and proper record-keeping.
By understanding these legal aspects, nurses can utilize the Brain Nursing Report Sheet responsibly while safeguarding their patients' rights and health information.