


Definition & Meaning of Authorization - Release Of Medical Records Information
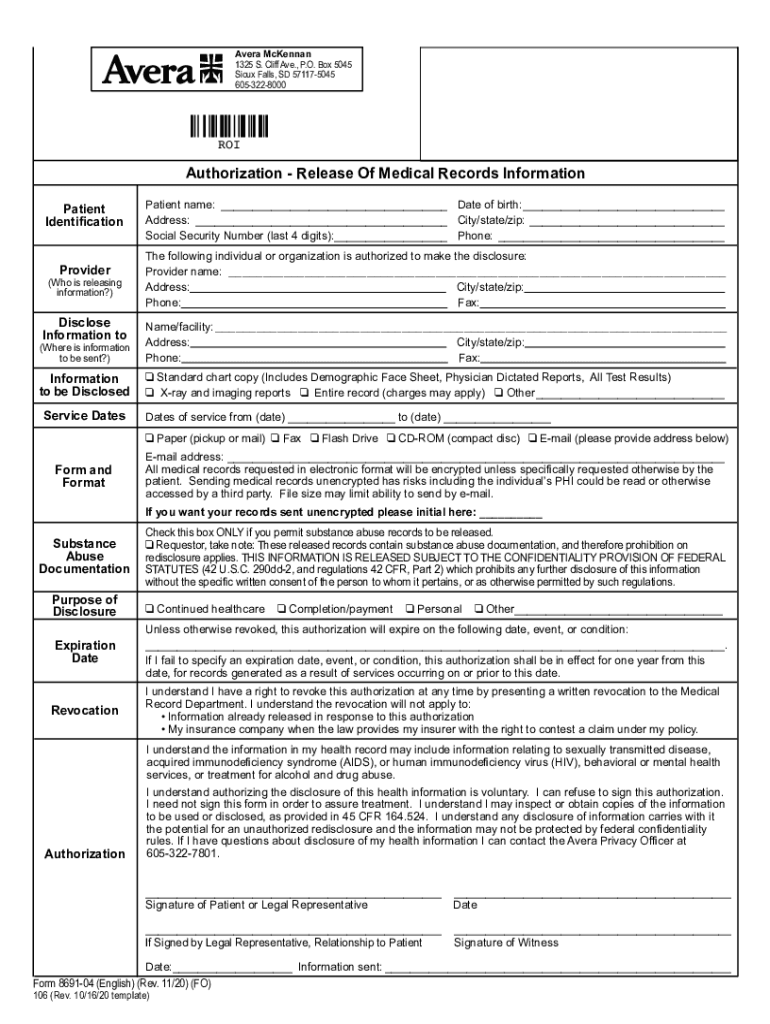
The "Authorization - Release Of Medical Records Information" is a legally binding document that enables a patient to permit healthcare providers, such as hospitals or clinics, to share their medical data with specified third parties. This could include transferring medical records to another healthcare provider, insurance company, or a legal representative. The form is essential for maintaining patient privacy while ensuring necessary information is available to those involved in the patient's care or legal matters. Typically, this form includes sections for identifying the patient, detailing what information can be released, specifying the recipient, and outlining the purpose of the disclosure.
How to Use the Authorization - Release Of Medical Records Information
Utilizing the form effectively requires a clear understanding of its sections and ensuring that all details are accurately filled out. First, provide accurate patient identification, including full name, date of birth, and social security number if required. Next, identify the healthcare provider or institution responsible for storing the medical records. Specify the entities authorized to receive the information, ensuring their addresses and contact information are correct. Outline the types of information to be disclosed and any exceptions or limits. Sign and date the form to validate the authorization.
Practical Scenarios
- Transfer of Care: When changing healthcare providers, this form allows the seamless transfer of medical histories to continue appropriate treatment.
- Insurance Claims: For processing claims, insurers may require access to medical records; this form authorizes the release of necessary information.
- Legal Proceedings: In cases involving medical evidence, patients may authorize their legal representatives to obtain pertinent medical documents.
Steps to Complete the Authorization - Release Of Medical Records Information
Filling out the form requires several detailed actions to ensure compliance and privacy regulations are followed.
- Identify the Patient: Fill in patient details, ensuring clarity and precision to avoid processing delays.
- Specify the Healthcare Provider: List the institution or doctors who hold the records, including contact information.
- Define Recipients: Document the individuals or entities authorized to receive the records. Ensure their contact details are complete and correct.
- Detail Information to be Released: Specify which medical records can be disclosed, such as test results, diagnosis, treatment records, or physician notes.
- State the Purpose: Clearly articulate why the records are being released, e.g., "for continued care" or "legal evidence."
- Sign and Date: Both the patient and, if applicable, legal representatives must sign the document to make it valid.
- Submit the Form: Send the completed form to the healthcare provider responsible for the records.
Critical Considerations
- Ensure all sections are filled out completely. Incomplete forms may lead to delays.
- Keep a copy of the signed form for personal records.
- Confirm receipt with the healthcare provider to whom the form was submitted.
Legal Use of the Authorization - Release Of Medical Records Information
This form is critical in maintaining patient privacy rights under laws such as the Health Insurance Portability and Accountability Act (HIPAA) in the United States. It provides a legal framework for safeguarding sensitive health information, ensuring that medical records are only shared with authorized parties. Legal safeguards attached to this document serve both patients and healthcare providers by clearly defining the permissible scope of record sharing. Breaches can result in severe penalties, both civil and criminal, for unauthorized disclosures.
Permissions & Restrictions
- Revocation Rights: Patients have the right to revoke authorization in writing unless information has already been disclosed.
- Scope Limitations: Only information outlined may be shared, ensuring patient control over personal data.
Key Elements of the Authorization - Release Of Medical Records Information
This form is composed of several critical components, each serving a unique purpose in ensuring the efficient and lawful exchange of medical information.
Main Components:
- Patient Information: Includes personal identification details.
- Provider Information: Details about the healthcare institution or provider holding the medical records.
- Recipient Details: Information on the person or organization receiving the data.
- Types of Information: Specific details about what medical records can be released.
- Purpose of Disclosure: The reason for releasing the information, such as transferring care or legal needs.
- Authorization Dates: Include the start and expiration date of the authorization.
State-Specific Rules for Authorization - Release Of Medical Records Information
While the general structure of the form remains consistent across the United States, certain state-specific rules may apply, especially concerning additional privacy protections or specific content requirements per state law.
Examples of Variations
- California: Has stringent privacy laws requiring specific language related to mental health records.
- Massachusetts: May demand additional consent for HIV/AIDS-related information.
- New York: Limits the time period during which records can be disclosed, necessitating more frequent renewals of authorization.
It is crucial for patients and healthcare providers to be aware of these variations to ensure compliance with local regulations.
Important Terms Related to Authorization - Release Of Medical Records Information
Understanding the terminology used in this context is vital for proper form completion and ensuring that all parties are clear on the agreement's scope.
Key Terms:
- Authorization: A patient's consent to release medical information.
- Confidentiality: The principle of keeping patient information private.
- Disclosure: The act of releasing or exposing information to another party.
- Revocation: The process of withdrawing consent, effectively nullifying the authorization.
These terms play a significant role in the management and sharing of sensitive health information. Mastery of this vocabulary helps in navigating the requirements and rights associated with medical records authorization.