


Definition & Meaning
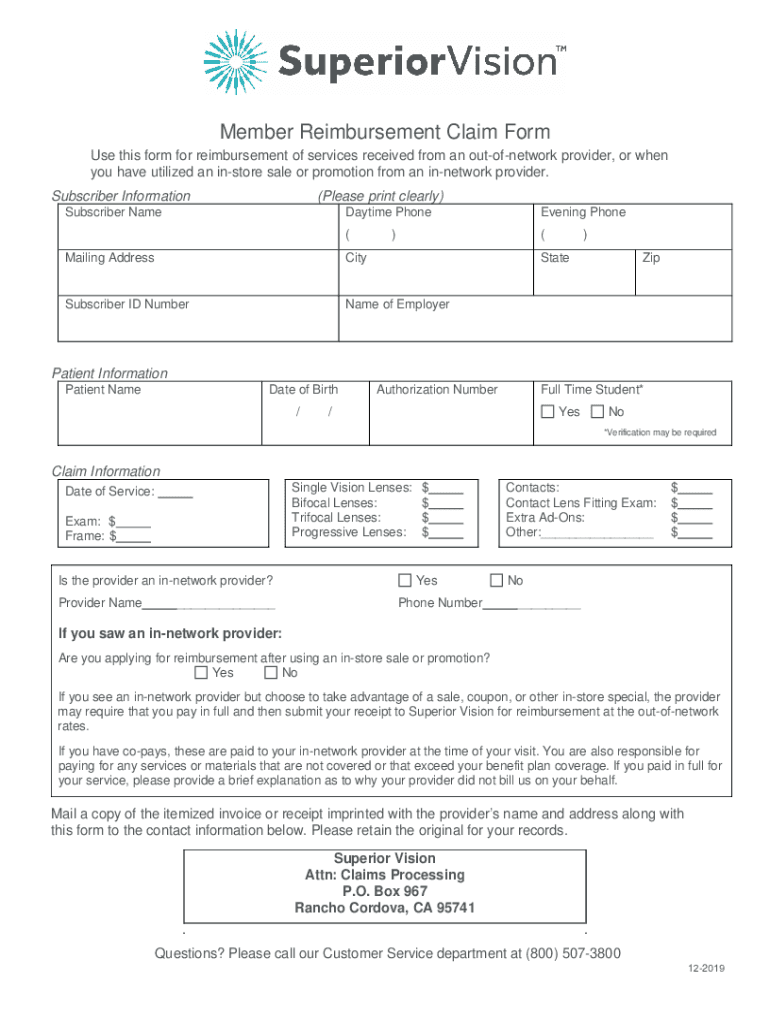
The "Member Reimbursement Claim Form - AllWays Health Partners" is a crucial document used by members to request financial reimbursement after receiving medical services from out-of-network providers or participating in in-store promotions with in-network providers. This form captures detailed information about the subscriber and patient, as well as specifics regarding the medical services or purchases for which reimbursement is sought.
The form's primary function is to facilitate the refund of out-of-pocket expenses incurred by members, ensuring that health-related financial transactions are transparent and properly documented. Adhering to this standardized format helps streamline the reimbursement process and provides clarity for both the member and AllWays Health Partners.
Key Elements of the Form
The Member Reimbursement Claim Form includes several important sections that must be filled out accurately:
-
Subscriber Information: This part of the form requests details such as the member's name, address, and unique identification number associated with their AllWays Health Partners account.
-
Patient Information: It covers details about the patient receiving the service, which may include age, relationship to the subscriber, and the type of insurance coverage held.
-
Claim Details: Members must provide comprehensive information about the service received. This includes the date of service, type of service, out-of-pocket amount paid, and the provider's name and address.
-
Submission Instructions: This section outlines how to compile and submit necessary documents, like itemized invoices or receipts, to ensure the claim is processed effectively.
Steps to Complete the Form
Filling out the Member Reimbursement Claim Form accurately is essential. Here are steps to guide you through the process:
-
Gather Required Information: Prepare necessary documents like your insurance card, receipts, and itemized invoices.
-
Complete Subscriber Information: Enter all required details about the policyholder, ensuring accuracy in names and addresses for proper identification.
-
Fill in Patient Information: Describe the patient's details as requested, making sure the relationship to the subscriber is clearly defined.
-
Enter Claim Information: Provide detailed descriptions of the services rendered, ensuring dates, service types, amounts, and provider information are correct.
-
Attach Supporting Documents: Include copies of receipts, invoices, and any additional documentation that substantiates your claim.
-
Submit the Form: Follow the submission instructions precisely. This might involve mailing the completed form and supporting documents to a specified address or using an online submission portal.
Who Typically Uses the Form
This form is predominantly used by members of AllWays Health Partners who have received medical services outside of their network but still want to benefit from their healthcare plan’s reimbursement provision. Typical users include:
-
Patients Seeking Reimbursement: Those who have incurred expenses from out-of-network providers.
-
Healthcare Subscribers: Subscribers who use in-store promotions and need to report these for reimbursement.
-
Caregivers: Individuals filing on behalf of a patient, such as a parent or legal guardian.

Eligibility Criteria
To ensure your claim is processed, certain conditions must be met:
-
Active Coverage: You must be an active member of AllWays Health Partners during the time of the service to be eligible for reimbursement.
-
Service Location and Type: Review the policy to confirm if the out-of-network service or in-store promotion is eligible for reimbursement.
-
Financial Responsibility: Only services that have been fully paid by the member, without having claims already submitted to AllWays Health Partners, qualify for reimbursement.

Important Terms Related to the Form
Understanding the critical terms associated with this form can help ensure accuracy:
-
Out-of-Network Provider: Refers to service providers not contracted under the member’s health plan.
-
Reimbursement: The process of compensating an individual for expenses already claimed and paid out-of-pocket.
-
Itemized Invoice: A detailed bill from a service provider listing each service rendered, including costs.
-
Subscriber: The primary individual covered under the insurance plan.
Form Submission Methods
The form offers flexibility in submission to accommodate different preferences and circumstances:
-
Mail Submission: Members can choose to send the completed form along with necessary documentation via postal mail, making sure it is addressed correctly to the claims department of AllWays Health Partners.
-
Online Submission: Some forms offer an electronic submission option, where members can fill out and upload the form and supporting documents through the health partner’s designated portal, streamlining the process and reducing mail transit times.
Required Documents
Ensure you gather and include the following documents with your form submission:
-
Copy of Itemized Invoices: Detailing the service provided, date of service, and breakdown of charges.
-
Receipts: Proof of payment showing the exact amount paid out-of-pocket.
-
Insurance Card Copy: A front-and-back photocopy of your AllWays Health Partners insurance card for verification purposes.