Definition & Meaning
The "24 h on claim form" refers to a specific document utilized in certain jurisdictions for procedures related to emergency detention, medical evaluation, or claims processing within a 24-hour window. Typically, these forms are used in contexts where rapid action is essential, such as mental health evaluations or insurance claims requiring immediate attention. The form's structure usually includes fields for key information that must be submitted or verified quickly to prevent any lapses in procedural or legal requirements.
How to Use the 24 h on Claim Form
To effectively use the "24 h on claim form," it's essential to understand its purpose and the specific information it requires. Users should begin by carefully reading any instructions or guidelines accompanying the form, as these provide critical insights into how to accurately complete and submit it. Often, the form will prompt users to fill in information such as personal identification details, specific events, or justifications for claims. In some instances, additional evidence or documentation may be needed to support the data provided.
Step-by-Step Completion Process
-
Review the Form: Before entering any information, familiarize yourself with all sections to understand what is required.
-
Gather Required Information: Collect all necessary details and documents, which may include identification numbers, medical records, or other essential paperwork.
-
Fill Out the Form: Enter the required data accurately, ensuring all fields are completed as instructed.
-
Attach Supporting Documents: Include any necessary attachments that support your claim or request.
-
Verify Accuracy: Double-check all entries for errors or omissions to prevent processing delays.
-
Submit the Form: Depending on the form's requirements, this might involve mailing it to a specified address, submitting it online, or delivering it in person.
Important Terms Related to the 24 h on Claim Form
Understanding key terminology can significantly ease the process of completing a 24-hour claim form. Terms often encompass specific codes or jargon unique to the form's context, such as medical or insurance terms.
- Emergency Detention: A legal hold allowing for the temporary confinement of individuals considered a risk.
- Claimant: The individual or party submitting the form.
- Evaluation Period: The 24-hour timeframe during which actions or decisions must occur.
- Evidence Required: Supporting documents or records needed to verify claims or statements made within the form.
Key Elements of the 24 h on Claim Form
Each section of the form plays a critical role in the submission process. Key components might include:
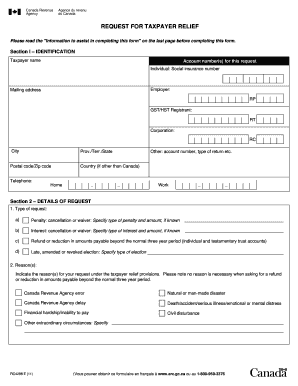
- Identification Information: Fields requiring personal details such as name, address, and contact information.
- Incident or Claim Description: A section detailing the specific event or reason for submitting the form.
- Verification Field: An area for authorized personnel to verify and approve the information provided.
- Signature and Date: Required for legal acknowledgment and tracking the form's submission date.
Legal Use of the 24 h on Claim Form
The legal utilization of a 24-hour claim form is crucial to ensuring compliance with regional or institutional regulations. It often involves:
- Authorization: Forms usually need authorized signatures to be considered legally valid.
- Confidentiality: Personal data included in the form must comply with privacy laws and be protected from unauthorized access.
- Regulatory Compliance: Ensuring all procedures align with applicable laws, such as those governing mental health interventions or insurance protocols.
How to Obtain the 24 h on Claim Form
Obtaining this form can vary depending on the jurisdiction and purpose. Common avenues include:
- Government Websites: Many jurisdictions offer downloadable forms through official portals.
- Institutional Sources: Relevant agencies or institutions may provide forms directly upon request.
- Online Services: Some platforms allow for online completion and submission of similar forms.
Required Documents
When completing a 24-hour claim form, additional documents are often necessary to provide verification and support. Typical documentation might include:
- Identity Verification: Copies of official identification like a driver's license or passport.
- Incident Reports: Relevant reports or documentation detailing the circumstances related to the claim.
- Proof of Condition or Incident: Any additional records or certifications that substantiate the claim, such as medical records or statements from professionals.
Form Submission Methods (Online / Mail / In-Person)
Submitting the completed form correctly is as vital as filling it out accurately. Available methods typically include:
- Online Submission: Digital upload through a secure portal, often requiring account authentication.
- Mailing: Sending the form and accompanying documents via certified mail to ensure secure and trackable delivery.
- In-Person Submission: Filing the form directly at a designated office, which may offer the opportunity for immediate review and feedback.