Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
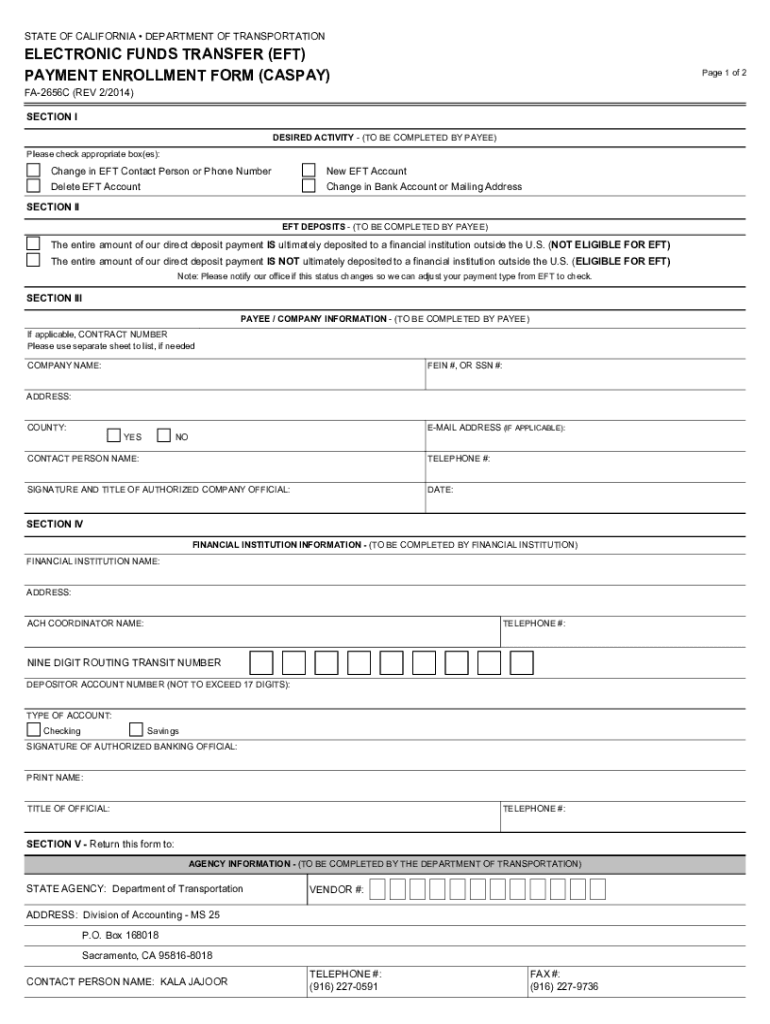
How to use or fill out Electronic Funds Transfer (EFT) Payment Enrollment Form
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open it in the editor.
In Section I, indicate your desired activity by checking the appropriate box. This could be a new EFT account, a change in contact information, or deletion of an existing account.
Move to Section II and select whether your direct deposit payment is ultimately deposited outside the U.S. This is crucial for determining eligibility for EFT.
In Section III, provide your company information including name, address, FEIN or SSN, and contact details. Ensure that the authorized official signs and dates this section.
Section IV requires your financial institution to fill in their details. They must include the routing number and account number while indicating the type of account (checking or savings).
Finally, ensure that all sections are completed accurately before submitting the form as instructed in Section V.
Start using our platform today to streamline your EFT Payment Enrollment process for free!
Fill out Electronic Funds Transfer (EFT) Payment Enrollment Form online It's free
See more Electronic Funds Transfer (EFT) Payment Enrollment Form versions
We've got more versions of the Electronic Funds Transfer (EFT) Payment Enrollment Form form. Select the right Electronic Funds Transfer (EFT) Payment Enrollment Form version from the list and start editing it straight away!
Enroll in automatic payments Authorizing Electronic Funds Transfer (or EFT) as your payment method will speed payment delivery by depositing payments directly to your bank account, allowing quicker access to funds paid to you.
What is an EFT form used for?
Electronic funds transfers (EFTs) are transactions that move funds electronically between different financial institutions, bank accounts, or individuals. EFTs are frequently referred to as electronic bank transfers, e-checks, or electronic payments.
Who needs to fill out an EFT form?
Organizations choosing to pay by EFT must submit an Electronic Funds Transfer Authorization form before EFT payments can be processed. Only a Data Bank administrator can authorize, modify, or terminate your organizations EFT account.
What is an EFT enrollment form?
Use this form to enroll in Direct Deposit of your federal payment from the General Services Administration. Last Name. First Name.
How to get proof of EFT?
The EFT trace number is typically found on the transaction details or confirmation receipt provided by the bank or payment processor. It can also be located in your bank statement under the specific EFT transaction, helping to identify and track the transfer within the banking system.
Related Searches
Electronic funds transfer eft payment enrollment form templateElectronic funds transfer eft payment enrollment form pdfElectronic funds transfer eft payment enrollment form onlineElectronic funds transfer eft authorization agreement cms 588Electronic funds transfer eft payment enrollment form californiaFree EFT form PDFFree EFT Authorization form templateEFT form for direct deposit
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Electronic Payments This requirement includes payments made to community medical and dental providers. Community care providers must enroll for Electronic Funds Transfer (EFT) in order to meet this requirement. With EFT, payments are deposited directly into a bank account.
Related links
Electronic Fund Transf - OperationsCommander (OPSCOM)
If you will be using EFT as a payment method, you must provide Tomahawk with the client number. This is provided by the Royal Bank and will be the identifierRead more
Electronic Funds Transfer (EFT) Payment Enrollment Form
Electronic Funds Transfer (EFT) Payment. Enrollment Form. This form is used for Automated Clearing House (ACH) payments with an addendum record that containsRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.