Start using our platform today to easily complete your masshealth necessity form online for free!
Sure, and it’s really straightforward! DocHub is an online PDF editor with advanced document processing functions that allow you quickly modify your documents, fill out empty fields and insert new ones for other people to fill out, and create eSignatures in several ways. Upload your dme form fill, provide information as requested, and decide how you want to eSign your template - by typing your name, drawing your signature, uploading its image, or utilizing a QR code.
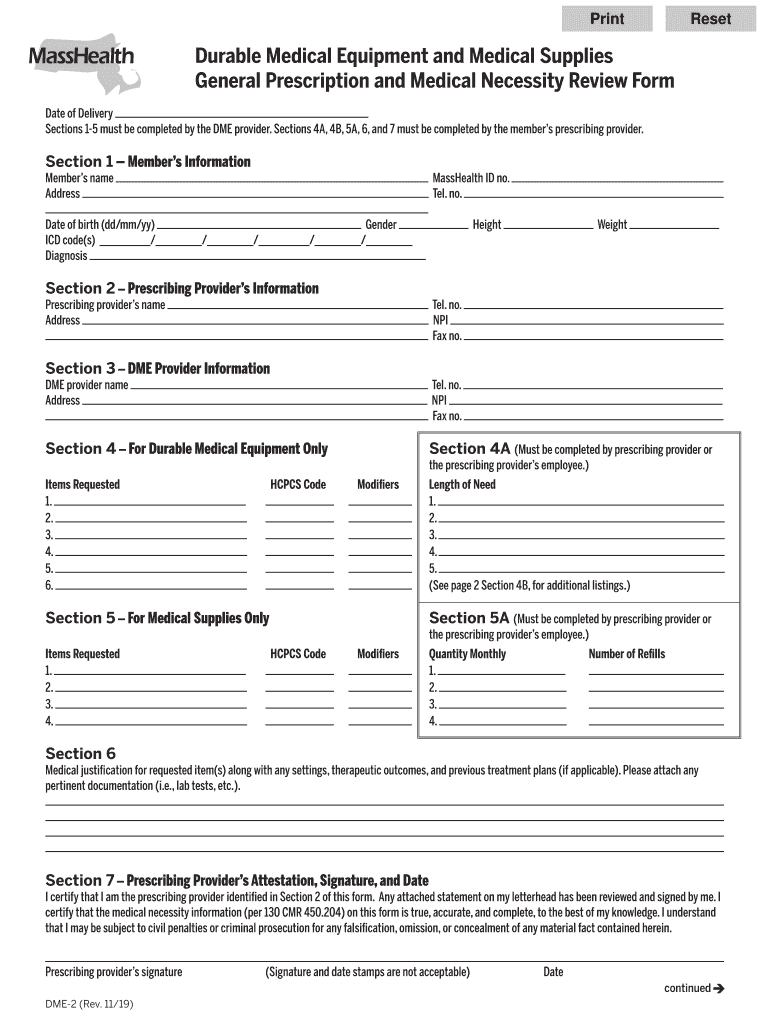
You can find the latest and most relevant version of the dme form pdf in our DocHub forms library. Browse it by categories or utilize the search field to find the exact template that suits your case. You may open this form for editing once you find it.
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Learn more