Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out doctors claim form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
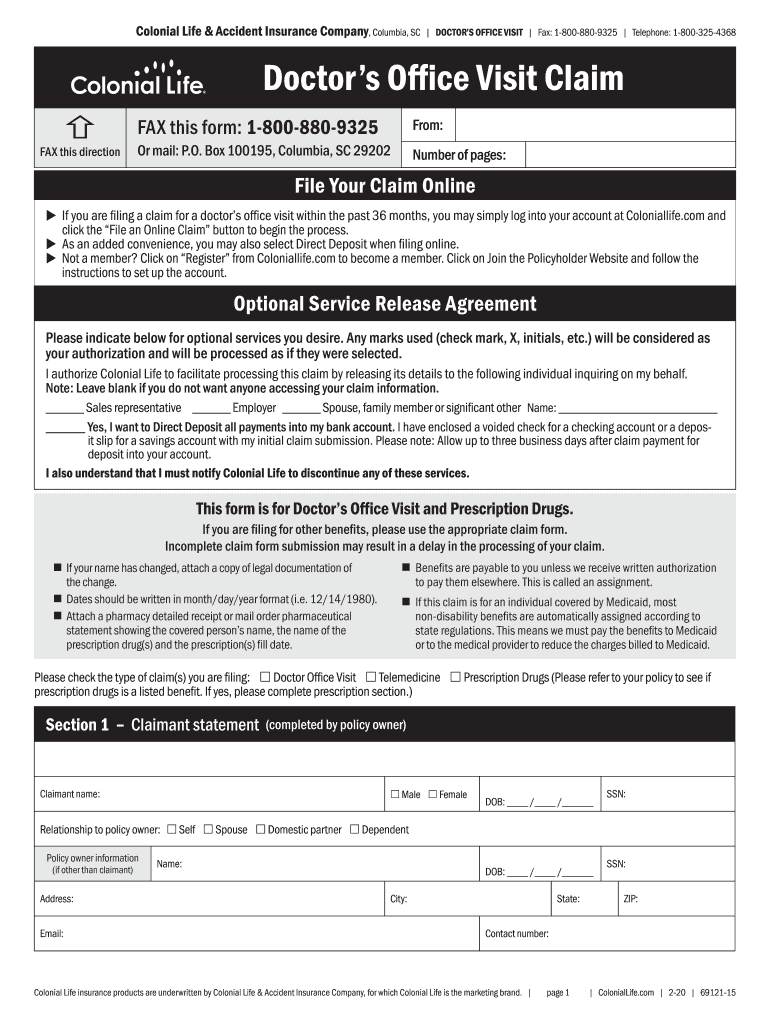
Click ‘Get Form’ to open the Doctor's Office Visit Claim in the editor.
Begin by filling out the Claimant Statement section. Enter the claimant's name, date of birth, and Social Security Number (SSN). Indicate the relationship to the policy owner.
In the Policy Owner Information section, provide details such as name, address, email, and SSN if different from the claimant.
Specify the type of claims you are filing by checking the appropriate boxes for Doctor Office Visit, Telemedicine, or Prescription Drugs.
Complete the visit details for each physician or facility visited. Include dates of visits and check whether they were in-office or telemedicine appointments.
If applicable, fill out the prescriptions section by providing pharmacy names, prescription numbers, and dates filled. Attach copies of receipts.
Review all entries for accuracy. Sign and date where indicated to certify that all information is correct before submitting your claim.
Start using our platform today to streamline your claims process for free!
Doctors claim form templateDoctors claim form pdfDoctors claim form onlineHealth Insurance claim form PDFPrintable medical claim FORMPrintable CMS 1500 formHealth insurance claim form pdf freeHealth INSURANCE CLAIM FORM example
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
OWCP-1500 Health Insurance Claim Form For Medical Services. Claims filed under FECA are for employment-related illness or injury. all Doctors of Medicine (M.D.
MEDICAL CLAIM FORM. Claims Receipt Center. P.O. Box 211184. Eagan, MN 55121. TO BE COMPLETED BY PATIENT. PATIENT INFORMATION: 1. PATIENTS NAME. (LAST). (FIRST).Read more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.