Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send form cms l564 via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out cms l564 with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
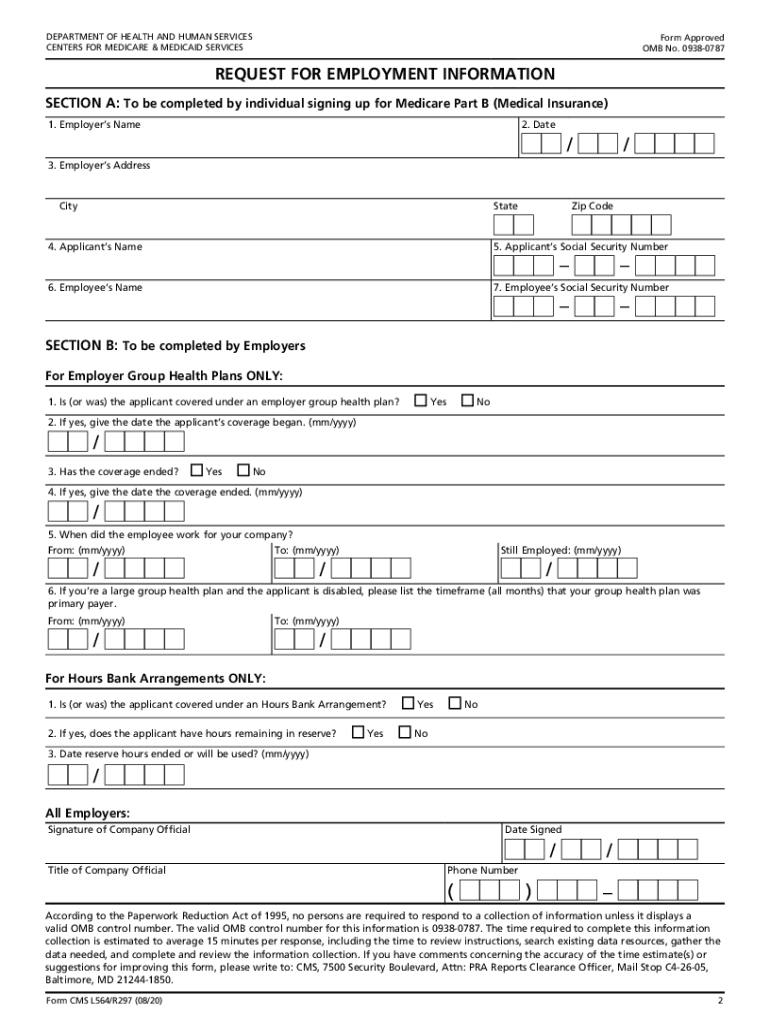
Click ‘Get Form’ to open the cms l564 in the editor.
In Section A, fill in your employer’s name, date, and address. Then, provide your name and Social Security Number, along with the employee's details if applicable.
Once you complete Section A, share the form with your employer for them to fill out Section B.
In Section B, your employer will confirm coverage details and employment dates. Ensure they sign and date the form before returning it.
After both sections are completed, submit the cms l564 along with your Medicare application to your local Social Security office.
Start using our platform today for free to streamline your form completion process!
The Centers for Medicare and Medicaid Services (CMS) provides health coverage to more than 100 million people through Medicare, Medicaid, the Childrens Health Insurance Program, and the Health Insurance Marketplace.
What is the CMS form used for hospital billing?
The Form CMS-L564 is used for proof of group health plan coverage based on current employment (i.e., active coverage), which is needed to process the Medicare enrollment application.
What type of insurance is CMS?
The rule enhances certain policies from the CMS Interoperability and Patient Access Final Rule (CMS-9115-F) and adds several new provisions to increase data sharing and reduce overall payer, healthcare provider, and patient burden through improvements to prior authorization practices and data exchange practices.
What is form CMS L564?
This form is used for proof of group health care coverage based on current employment. This information is needed to process your Medicare enrollment application. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment.
cms l564 form
Cms l564 form pdfCMS-40BCMS-L564 form DownloadCMS L564 Request for Employment InformationPrintable CMS L564 form downloadCMS-L564 form for spouseCMS L564 2026CMS-L564 form online
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Form CMS-L564 (Revised 03/2025). Medicare Request for Employment Information. Use this form to show proof of group health plan coverage based on currentRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.