Overview of the Sanofi Patient Assistance Refill Form
The Sanofi patient assistance refill form plays a critical role in enabling patients to access their essential medications, particularly for those who may struggle with the costs. This program supports individuals who require ongoing treatment through financial assistance. The following sections break down important details related to the form, including usage, eligibility, and required documentation.
Purpose of the Sanofi Patient Assistance Refill Form
The form serves as a crucial tool for patients to request refills of their medications provided through the Sanofi Patient Assistance Program (PAP). This program is dedicated to helping uninsured or underinsured patients obtain necessary medications at little to no cost. The refill form specifically ensures that patients can maintain their treatment regimens without interruption. Key aspects include:
- Medication continuity: Ensuring refills occur promptly to avoid treatment delays.
- Streamlined processes: Simplifying the application and refill request procedures for patients and healthcare providers.
- Accessibility: Making it easier for patients to fill out the required information, thus facilitating quicker access to medications.
Eligibility Criteria for the Sanofi Assistance Program
Potential applicants must meet certain criteria to qualify for assistance through the Sanofi patient assistance program. Common eligibility factors include:
- Income requirements: Applicants should demonstrate financial need, typically based on household income relative to the federal poverty level.
- Insurance status: The program is aimed at individuals without insurance, or those whose insurance does not cover the prescribed medications.
- Healthcare provider involvement: Patients must have prescriptions from a licensed healthcare provider, who may need to submit additional information as part of the refill process.
It's crucial for applicants to familiarize themselves with these criteria to ensure a smooth application process.

Documentation Required for Submission
When completing the Sanofi patient assistance refill form, several types of documentation may be required. This ensures the program can accurately assess eligibility and process refills expediently. Required documents may include:
- Proof of income: Recent pay stubs, tax returns, or government assistance documentation to verify income levels.
- Current insurance information: If applicable, details about any existing coverage and what medications may not be covered.
- Healthcare provider’s prescription: A valid prescription for the medication needing a refill, often required to be filled out or supplemented by a healthcare professional.
Providing complete documentation increases the likelihood of successful approval.
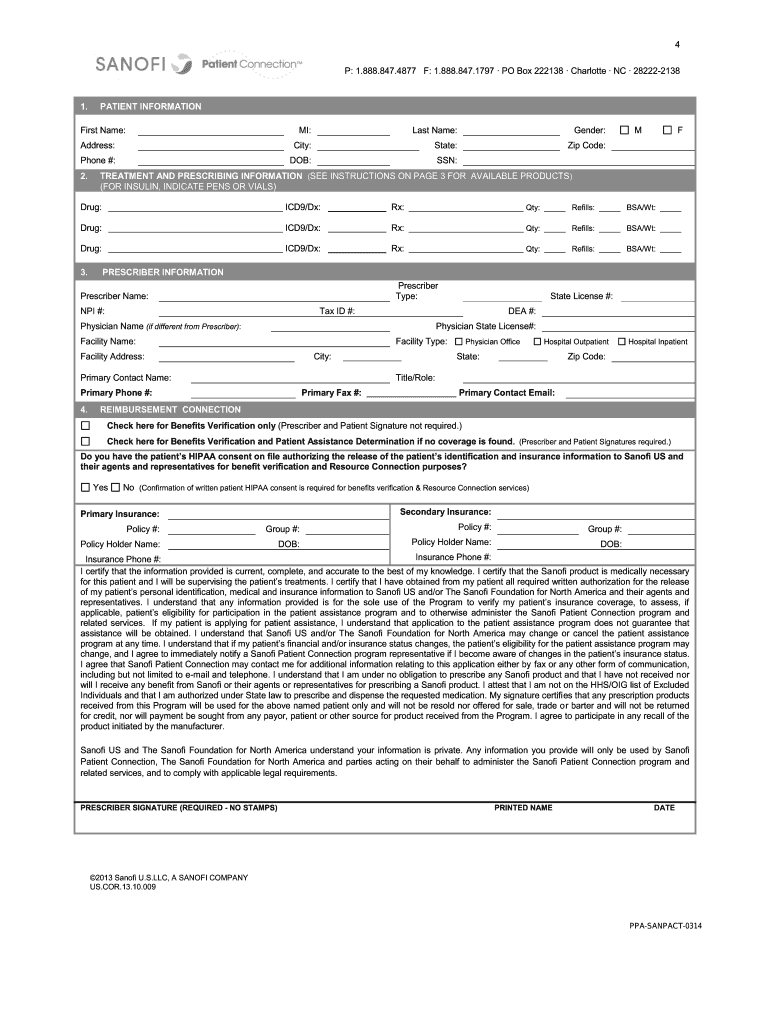
How to Use the Sanofi Patient Assistance Refill Form
Filling out the refill form accurately is essential to expedite the assistance process. Here’s a step-by-step guide to using the form effectively:
- Obtain the form: Access the Sanofi patient assistance refill form, typically available online or through healthcare providers.
- Complete patient information: Fill in personal details, including full name, address, date of birth, and contact information.
- Medication details: Clearly indicate the name of the medication needed, dosage, and any relevant treatment history.
- Attach necessary documentation: Ensure all required documents are included to prevent delays in processing.
- Submit the form: Send the completed refill form and documents through the specified methods—usually online, by mail, or through a participating healthcare provider.
By following these steps, patients can streamline the refill request process.
Submission Methods for the Refill Form
Patients have multiple options for submitting the Sanofi patient assistance refill form, each catering to different preferences and situations. Common submission methods include:
- Online submission: If available, many patients prefer submitting their forms through an online portal, which is often quicker and allows for immediate confirmation of receipt.
- Mail: Patients can also print the completed form and send it via postal service to the designated address.
- Through healthcare providers: In some cases, healthcare providers can assist with the submission, allowing for coordinated care and efficient entry into the program.
Each method may have specific guidelines and processing times associated, so it’s essential to choose the most appropriate option based on individual circumstances.
Additional Resources for Patients
Patients looking for further assistance while navigating the Sanofi patient assistance refill form can leverage additional resources. These may include:
- Sanofi patient assistance phone number: A dedicated line can provide personalized guidance and answer any questions regarding the refill process.
- Patient advocacy groups: Organizations that specialize in pharmaceutical assistance may offer resources and support for understanding eligibility and application procedures.
- Healthcare provider support: Providers can assist with completing the form and ensuring that patients meet the necessary qualifications.
Utilizing these resources can enhance the likelihood of successful applications and timely medication access.