Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send medical necessity appeal letter example via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out medical necessity appeal letter template pdf with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
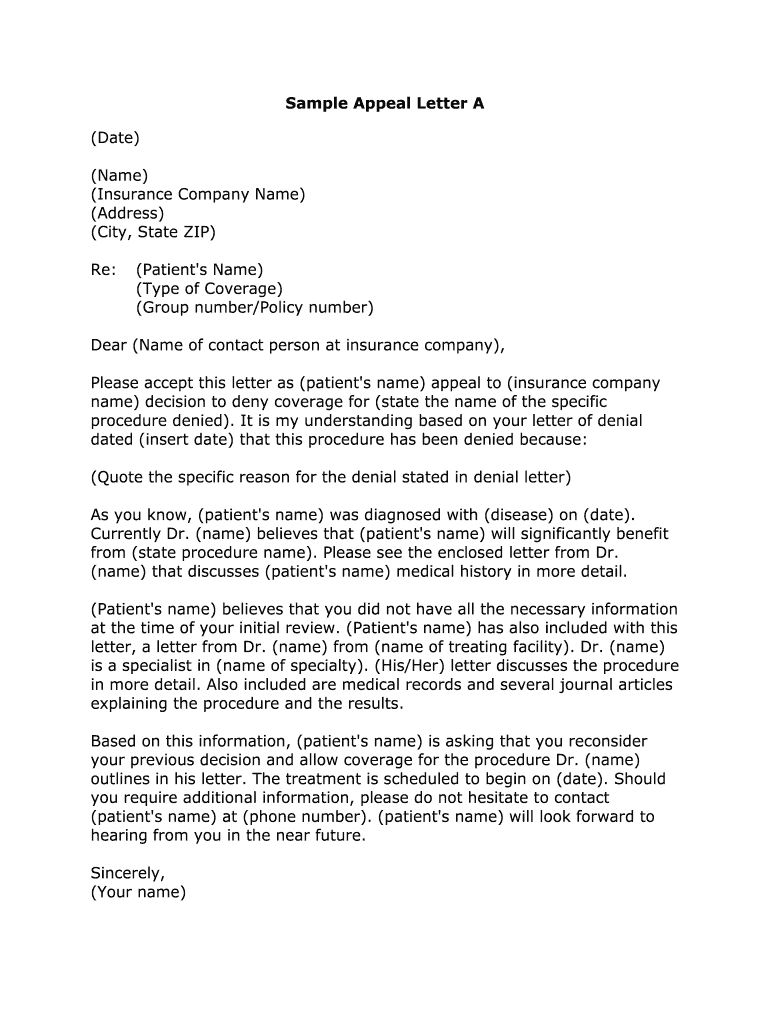
Click ‘Get Form’ to open the medical necessity appeal letter template in the editor.
Begin by entering the date at the top of the letter. This sets a clear timeline for your appeal.
Fill in your name and the insurance company’s name, along with their address and city, state, and ZIP code. Accurate contact information is crucial for effective communication.
In the 'Re:' section, input the patient's name, type of coverage, and group/policy number. This information helps identify the specific case being appealed.
Craft a personalized greeting using the contact person's name at the insurance company. If unknown, a general greeting can suffice.
Clearly state the reason for your appeal by quoting from the denial letter. This establishes context for your request.
Provide details about the patient’s diagnosis and how they will benefit from the denied procedure. Include supporting documents as necessary.
Conclude with a polite request for reconsideration and provide contact information for follow-up. Ensure all fields are filled accurately before finalizing.
Start editing your medical necessity appeal letter today on our platform for free!
Fill out medical necessity appeal letter template pdf online It's free
What is an example of a medical necessity appeal letter?
Things to Include in Your Appeal Letter Patient name, policy number, and policy holder name. Accurate contact information for patient and policy holder. Date of denial letter, specifics on what was denied, and cited reason for denial. Doctor or medical providers name and contact information.
What is an example of a good appeal letter?
This includes a brief description of the patients diagnosis, the severity of the patients condition, prior treatments, the duration of each, responses to those treatments, the rationale for discontinuation, as well as other factors (eg underlying health issues, age) that have affected your treatment selection].
How do you write an effective medical appeal letter?
The explanation of benefits (EOB) letter from the health plan is the key to payment or denial status. If the coverage language supports payment, write an appeal letter describing the disorder and its medical nature, and reference the coverage policy paragraph that shows how your treatment fits coverage criteria.
How would you appeal a denial for medical necessity?
I am writing to appeal my current disciplinary status, and to apologize for my involvement in the floor crawl which led to my being placed on notice. I realize that what seemed harmless fun to me was actually a danger to my health and the health of others. I sincerely regret my actions that night
medical necessity appeal letter template
Medical necessity appeal letter template pdf freeSample Appeal letter for medication denial PDFFree medical Appeal Letter sampleMedical Necessity Appeal letter exampleMedical necessity appeal letter example for insuranceSample letter of appeal for reconsideration insurance claims PDFSample appeal letter for prior authorization denial PDFMedical Appeal letter template
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Example letter for a not medically necessary denial
Example letter for a not medically necessary denial. Situation: A medical provider billed you for a denied claim. You decide to appeal the denied claim.Read more
Medically Necessary or Medical Necessity: Services that include medical letter acknowledging their grievance, unless they have requested an expedited appealRead more
We believe that [name of service, procedure, or treatment sought] is medically necessary to treat [name of plan member if other than yourself]s medicalRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.