


Definition & Meaning of the Functional Abilities Form Template
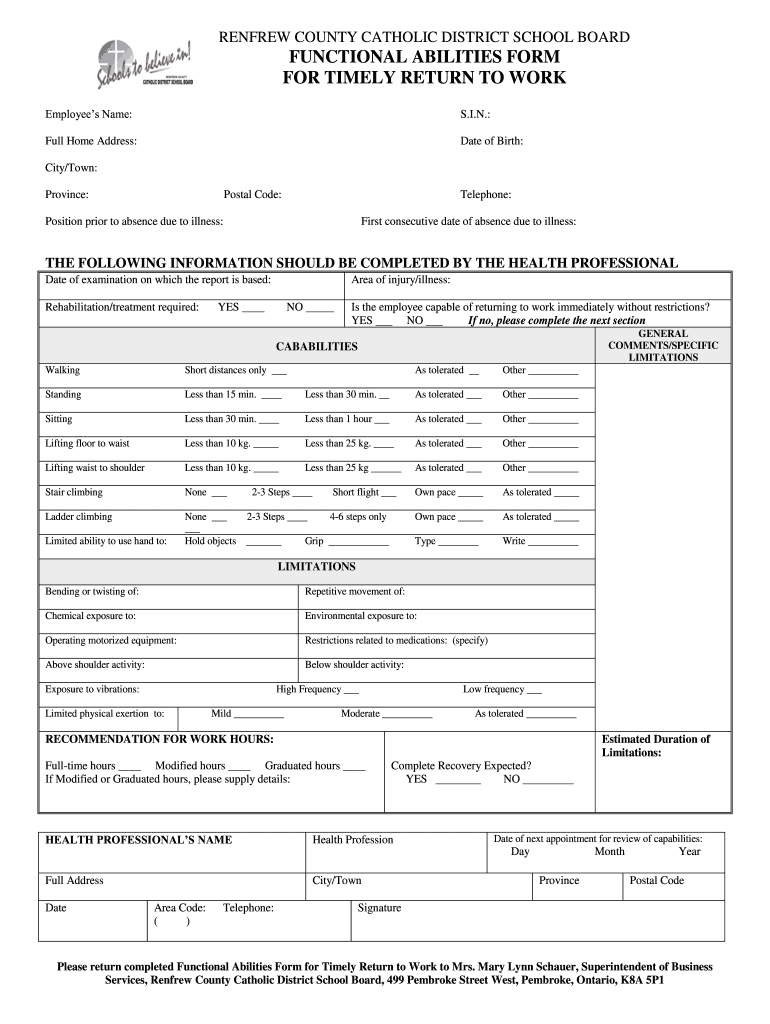
The functional abilities form template is a standardized document used to assess an individual's capacity to perform work-related tasks after any health-related absence. This form plays a crucial role in workplace reintegration, particularly after an employee has experienced illness or injury. It serves to outline an employee's physical capabilities and limitations, providing a clear framework for employers and health professionals to identify necessary accommodations or restrictions.
This form typically includes various sections dedicated to personal information, medical evaluations, and specific details on functional abilities. For example, the sections may request information about lifting capacity, endurance, mobility, and any specific restrictions related to the individual's condition. Overall, the functional abilities form template facilitates a seamless return to work for employees, ensuring that their health and safety are prioritized during the transition.
How to Use the Functional Abilities Form Template
Using the functional abilities form template involves several essential steps geared towards collecting accurate and comprehensive information about an employee’s physical capabilities. This process typically follows these stages:
- Obtain the Form: The template can usually be downloaded from organizational portals or HR departments. Ensure that the latest version is used.
- Complete Personal Information: Fill out the employee's name, contact information, job title, and department. This initial section helps identify the individual for whom the assessment is being conducted.
- Health Professional's Evaluation: A healthcare provider must review the employee’s medical history and current health status. They will complete the medical evaluation section, clearly indicating the employee's abilities and any restrictions.
- Functional Descriptions: Specify the task-related capabilities of the employee, including but not limited to lifting, standing, walking, and other job-specific functions.
- Signature and Date: Once completed, the form should be signed by both the healthcare provider and the employee, along with the date of completion, ensuring accountability and validity.
By following these steps, employers can obtain a comprehensive overview of the employee's health and necessary accommodations, leading to informed decisions regarding workplace adjustments.
Key Elements of the Functional Abilities Form Template
Several critical components define the structure and functionality of the functional abilities form template. These key elements encompass:
- Personal Information Section: Includes fields for the employee's name, contact details, and employment information.
- Medical Evaluation by Health Professional: A section dedicated to the healthcare provider’s assessment that includes a review of the individual’s medical condition.
- Functional Abilities: Detailed descriptions of physical capabilities such as lifting strength and mobility assessments, which are vital in determining work readiness.
- Limitations and Restrictions: Identifying any physical limitations or restrictions due to the health condition. This part is crucial for planning accommodations in the workplace.
- Accommodations Needed: Depending on the assessment, specific needs for workplace adjustments may be indicated to support the employee’s return to work safely.
Each of these elements contributes to a thorough understanding of the employee’s readiness to resume their role, ensuring compliance with workplace health and safety regulations.
Important Terms Related to the Functional Abilities Form Template
Understanding key terms related to the functional abilities form template helps clarify its purpose and usage:
- Workplace Accommodations: Adjustments made to a work environment that enable individuals with disabilities or health concerns to perform their job duties effectively.
- Functional Capacity Evaluation (FCE): A comprehensive assessment to determine an individual’s physical abilities and limitations in relation to specific job tasks.
- Return-to-Work Program: Structured plans aimed at facilitating the transition of employees back into the workplace post-injury or illness.
- Medical Certification: The documentation provided by a healthcare professional, confirming an employee's fitness for work or outlining necessary accommodations.
- Limitations: Specific activities or functions that an individual is unable to perform due to health issues, which directly impact their ability to fulfill job responsibilities.
Grasping these terms is crucial in navigating the procedural aspects of using the functional abilities form effectively.
State-Specific Rules for the Functional Abilities Form Template
It is vital to recognize that regulations regarding the completion and submission of the functional abilities form template can vary by state. Specific requirements may include:
- Documentation Standards: Some states may require additional documentation along with the functional abilities form, such as previous medical records or additional evaluations.
- Timeframes for Submission: Different states may have specified deadlines for when the form must be submitted post-injury or illness to ensure compliance with workplace safety regulations.
- Standardization: While the general template is widely used, specific states may implement unique adaptations or additional sections relevant to local laws and regulations.
Understanding these state-specific considerations ensures that employers and employees adhere to legal standards while facilitating a smooth transition back to work.
Examples of Using the Functional Abilities Form Template
Various scenarios illustrate the application of the functional abilities form template, showcasing its effectiveness in real-world settings:
-
Case Study: An employee recovering from knee surgery requires modifications to their work environment. After completing the functional abilities form, it is determined that the employee can perform desk duties but needs a sit-to-stand desk to accommodate their recovery needs.
-
Team Assessment: A team returning from a company-sponsored wellness initiative must complete functional abilities evaluations. This process highlights individual members’ capabilities and ensures that team dynamics are not disrupted due to unseen health concerns.
-
Policy Compliance: A company enforces a return-to-work policy that requires all employees coming back from medical leave to submit the functional abilities form. This measure not only protects the employees but also shields the employer from potential legal repercussions.
These examples showcase how the functional abilities form serves as a critical tool in promoting employee welfare while ensuring compliance with workplace regulations.